Tickborne Diseases
View Previous YearsDespite its urban setting, Philadelphia has one of the largest park systems in the country and is home to a variety of ticks, some of which are capable of spreading disease to humans. Lyme disease is endemic to Philadelphia, and residents have also tested positive for other tickborne infections including anaplasmosis, babesiosis, ehrlichiosis, and Rocky Mountain spotted fever with less frequency.
Click here for more information on tickborne disease
Philadelphia Lyme and Other Tickborne Disease Surveillance Update
Lyme Disease
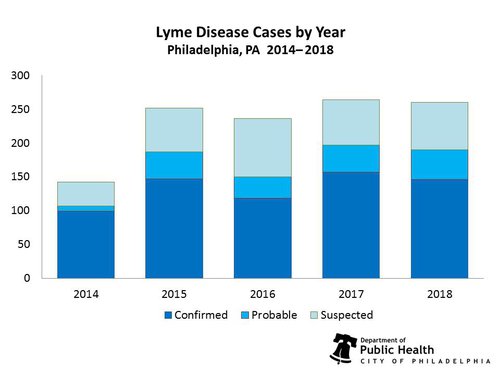
In 2018, the Philadelphia Department of Public Health (PDPH) received over 700 Lyme disease reports and identified 260 individuals with positive laboratory testing and/or clinical symptoms consistent with the infection. The number of people contracting Lyme disease in Philadelphia during 2018 was similar to that in 2017, though the actual number of infections is likely still underreported. It is important to remember that this disease is endemic to the area and preventative measures should be discussed with any patient who spends time outdoors.
Lyme Disease Cases by Year
Reported cases of lyme disease, 2014-2018
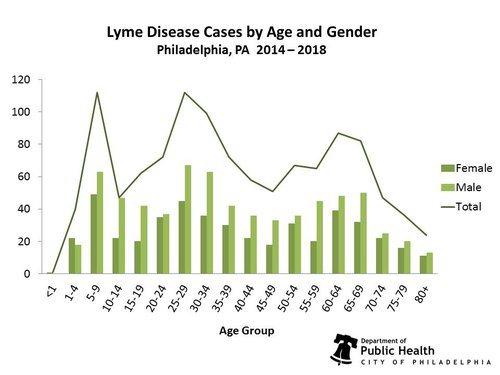
The majority of 2018 cases were male (60.4%), and while Lyme disease has been diagnosed in individuals of all ages, higher counts were reported in individuals 25-29 years old (10.8%). Higher counts were also seen in individuals 30-34 years old (10.4%), and both 5-9 and 65-69 years old (9.2%). These trends in age and gender for Lyme disease are similar to what PDPH has observed in the last 5 years.
Lyme Disease by Age and Gender
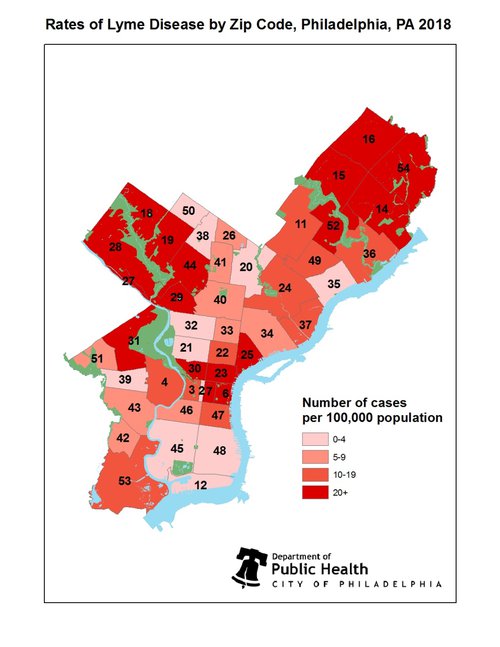
Cases of Lyme disease have been identified in nearly every ZIP code in Philadelphia, however more individuals living in close proximity to wooded areas like Wissahickon Valley Park and Pennypack Park were diagnosed with and/or tested positive for Lyme disease.
Rates of Lyme Disease by Zip Code, Philadelphia, PA 2018
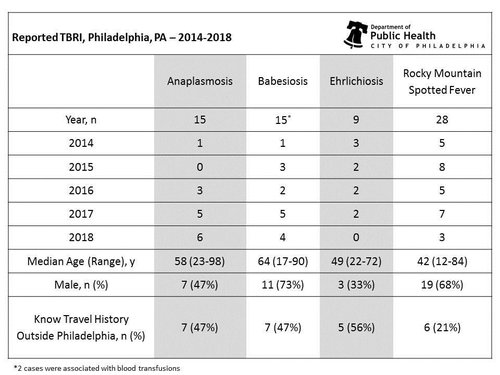
Other Tickborne Infections
The first locally-acquired case of babesiosis was identified by PDPH in 2013, and cases have been identified each year since. This supports the need to test patients for tickborne illnesses beyond Lyme disease. A summary of other tickborne infections identified by PDPH can be found in the table below.
Tick Surveillance
In 2012, the Pennsylvania Department of Environmental Protection (PA DEP) began collecting and testing ticks throughout the state to gain a better understanding of the number of ticks carrying pathogens capable of causing disease in humans. The PA DEP performed tick drags statewide, including Wissahickon Valley Park in Northwest Philadelphia and Pennypack Park in the Northeast. Since the fall of 2015, PDPH has performed additional tick drags at West Fairmount Park, Wissahickon Valley Park, Morris Park, and Tacony Creek Park. PA DEP performed pathogen testing on ticks collected in 2015 and 2016. Testing was unavailable for ticks collected in 2017 and is still pending for ticks collected in 2018. Of those tested, ticks positive for pathogenic organisms were identified at all collection sites, with a number of ticks co-infected with multiple pathogens. The presence of co-infected ticks demonstrates the need for comprehensive tickborne pathogen testing in patients suspected of having Lyme disease. It is important to note that in previous years, Philadelphia ticks tested positive for Babesia microti, providing evidence of the potential for local transmission of this parasite. A summary of the tick drag findings from 2016 and previous years can be found in the tables below.
 |
 |
Emerging Tickborne Infections
Blacklegged ticks, native to the Philadelphia area, are known vectors for many diseases. While cases of the following infections have not been identified in Philadelphia, they are important to consider for patients who may have been exposed to ticks. Emerging conditions can be reported under the unusual conditions mandate, and PDPH can help coordinate testing for these pathogens.
Powassan Virus
Powassan (POW) virus is a RNA virus that has two separate lineages in the United States, Lineage I (the “prototype” lineage) and Lineage II (also known as the Deer tick virus lineage). Both lineages of POW virus can be transmitted to humans through the bite of an infected tick. Lineage II is most commonly transmitted by Ixodes scapularis, which is native to the Philadelphia region. The virus is related to West Nile virus and is clinically similar, as patients present with fever, headache, vomiting, and signs of neurological impairment. Because of this similarity in presentation, diagnostic testing is an important tool in determining the cause of infection. The incubation period for POW virus ranges from 1 week to 1 month, and there is no specific treatment for infection aside from supportive care. Patients infected with POW virus can develop encephalitis and meningitis, with approximately 10% of encephalitis cases resulting in death. POW virus infection can cause permanent neurological deficits for approximately 50% of survivors, including recurrent headaches, muscle wasting, and memory loss. The first human case of POW virus in Pennsylvania was reported in 2011 in Lackawana County, though this infection may have been acquired outside of the state. While there have not been any reports of POW virus transmission in Philadelphia, locally-acquired cases have been reported in Pennsylvania. In 2018, 1 locally-acquired case was reported in Pennsylvania, and 4 cases were reported in 2017. Additionally, cases of POW virus have been identified in New York and New Jersey over the past 5 years.
Borrelia Miyamotoi
A spirochete closely related to that which causes tick-borne relapsing fever, B. miyamotoi has recently been implicated as a pathogen capable of causing disease in humans. Because cases of B. miyamotoi have been identified in the states surrounding Pennsylvania, and ticks capable of transmitting the bacterium (Ixodes scapularis) are endemic to Philadelphia, it is worth considering this pathogen as an important cause of illness. Most patients infected with B. miyamotoi experience headache, muscle aches, and recurring episodes of fever within 1 to 2 weeks of receiving a tick bite. Current testing is limited to PCR identification of the spirochete in serum and/or CSF collected at the time of illness. A two-week course of doxycycline has been effective in treating patients with known B. miyamotoi infections. If you suspect a patient may be infected with B. miyamotoi, PDPH is available to facilitate appropriate laboratory testing.
Ehrlichia muris-like
Ehrlichia muris eauclairensis is an obligate intracellular gram-negative bacterium. The majority of ehrlichiosis cases are caused by E. chaffeensis, followed by E. ewingii. E. muris eauclairensis was not implicated as a cause of human disease in the United States until 2009, when it was identified in the serum samples of patients with confirmed Ehrlichia infections who were living in Minnesota and Wisconsin. Individuals infected with E. muris eauclairensis can present with a variety of symptoms including fever, malaise, headache, nausea, and vomiting. The incubation period is between 1 and 2 weeks, with a median of 9 days. Common clinical laboratory findings include elevated liver enzyme levels, thrombocytopenia, and lymphocytopenia. While no cases of E. muris eauclairensis have been identified in Pennsylvania, Ixodes scapularis ticks are a known vector and could potentially transmit the bacteria locally.